
Open Journal of Clinical and
Medical Images
Research Article - Open Access, Volume 5
A case of emphysematous osteomyelitis of the calcaneus without concurrent subcutaneous emphysema
William Pacheco, DPM1*; Hadeel Zainah, MD2
1Resident, Department of Podiatric Medicine and Surgery, Kent Hospital, Warwick, RI, USA.
2Physician, Department of Infectious Disease, Kent Hospital, Warwick, RI, USA.
*Corresponding Author: William Pacheco
Resident, Department of Podiatric Medicine and Surgery, Kent Hospital, Warwick, RI, USA.
Email: wmpacheco15@gmail.com
Received : Sep 11, 2025
Accepted : Oct 06, 2025
Published : Oct 13, 2025
Archived : www.jclinmedimages.org
Copyright : © Pacheco W (2025).
Abstract
Emphysematous osteomyelitis is a rare, possibly fatal infection characterized by intraosseous air, most often associated with immunosuppression. We present an immunocompromised 68-year-old patient who has insulin dependent diabetes mellitus with neuropathy. He was found with emphysematous osteomyelitis of the calcaneus without concurrent subcutaneous emphysema with polymicrobial wound culture and bacteremia. Emphysematous osteomyelitis typically presents concurrently with subcutaneous emphysema in 79% of cases. Early detection is critical, as urgent surgical intervention and appropriate antibiotics are necessary to reduce morbidity and mortality.
Keywords: Emphysematous; Osteomyelitis; Intraosseous air; Necrotizing infection.
Citation: Pacheco W, Zainah H. A case of emphysematous osteomyelitis of the calcaneus without concurrent subcutaneous emphysema.Open J Clin Med Images. 2025; 5(2): 1210
Introduction
Emphysematous osteomyelitis is a rare variant of osteomyelitis that is defined by the presence of air within the intramedullary space [1]. There is sparse literature describing it, primarily consisting of case reports. The reported cases of infectious emphysematous osteomyelitis typically had comorbidities that led to immunocompromise, such as diabetes or malignancy [1-3,5]. Similar to subcutaneous emphysema formed by necrotizing soft tissue infections, emphysematous osteomyelitis needs prompt diagnosis and definite treatment due to its high mortality [1,2].
Our case report is of a 68-year-old male with insulin-dependent diabetes mellitus with emphysematous osteomyelitis of his calcaneus.
Case report
A 68-year-old male presented to our institution with concern for recurrent cellulitis to his left foot wounds. His medical history consisted of insulin-dependent diabetes with neuropathy, hypertension, peripheral vascular disease with previous revascularization, chronic left foot wounds, and multiple bilateral forefoot amputations, including a left-sided trans-metatarsal amputation. The patient has been seen at a local wound care center, where he had received 17 sessions of hyperbaric oxygen therapy and aggressive local wound care, including enzymatic debridement, sharp debridement, and negative pressure wound vac therapy for his chronic left rearfoot wounds.
He presented with generalized fatigue, decreased appetite, and acute lower quadrant pain with subjective complaints of a worsening left foot infection. His vital signs showed mild tachycardia of 103/min, blood pressure of 143/67 mmHg, temperature of 36.9°C, and respiratory rate of 16/min. Lower extremity examination consisted of handheld Doppler vascular assessment with monophasic signal to the anterior tibial, posterior tibial, and dorsalis pedis arteries. Increased warmth was present in the heel region. There was a medial heel and plantar lateral heel wounds that communicated within the deep tissue, separated by a full-thickness tissue bridge, with a mixed fibrogranular wound base (Figure 1). Both wounds probed to the plantar fascia and plantar calcaneal bone with surrounding erythema, along with malodorous mixed seropurulent drainage. Laboratory findings were significant for leukocytosis (17.0×10×3/mcL), Erythrocyte Sedimentation Rate elevation (51mm/hr), and hyperglycemia (217 mg/dL). Renal and liver function tests were normal. A culture of the deep wound and two sets of blood cultures were obtained. The patient was empirically started on empiric antibiotics of intravenous cefepime and vancomycin.
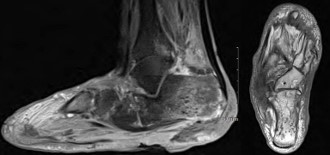
Left foot radiographs showed significant soft tissue defects and osteolysis within the inferior calcaneus, highly suspicious of underlying osteomyelitis (Figure 2). A Magnetic Resonance Imaging (MRI) of the left foot was ordered for further evaluation of underlying osteomyelitis. The result was concerning for osteomyelitis within the calcaneus with multiple punctate low signal foci suspicious of emphysematous osteomyelitis. The MRI also showed multiple fluid collections within the hindfoot and midfoot (Figure 3).
The patient underwent urgent left below-knee amputation. Pathology of the soft tissue and bone was without involvement of underlying osteomyelitis or inflammation; the microbiology of the surgical margins was without any growth. The wound culture showed polymicrobial growth consisting of MethicillinResistant Staphylococcus Aureus (MRSA), Pseudomonas aeruginosa, Enterococcus faecalis, Streptococcus viridans, and mixed gram-negative rods. One of the two initial blood cultures grew Streptococcus viridans and MRSA within the aerobic and anaerobic bottles. Enterococcus faecalis was also grown within the aerobic bottle. A transesophageal echocardiogram did not reveal vegetations, and the patient subsequently completed a four-week course of Linezolid. The patient had dehiscence of his incision site at approximately 1 month post-amputation, requiring surgical revision. Further follow up reveled a fully healed stump.
Discussion
Patients with diabetic foot ulcerations are at a significant risk of developing osteomyelitis, with literature supporting underlying bone infections being present in 10-15% of moderately infected diabetic ulcers and up to 50% in severe infections [4]. Patients with diabetic ulcers and developing osteomyelitis have a significant risk of amputation, which can be detrimental to a patient’s overall quality of life. Major amputations are a high risk, especially when diabetic ulcers are present on the rear foot, with approximately 50% undergoing a proximal amputation [4]. Emphysematous osteomyelitis presents a more challenging situation for clinicians, with Leuy et al. reporting that 15 of their 25 cases required surgical intervention, and 32% of patients did not survive in the hospital 7-56 days after diagnosis [3].
Emphysematous osteomyelitis is exceptionally rare, with potentially fatal consequences if not properly identified quickly [1,2,5]. Plain radiographs do not play a reliable role with a high incidence of false-negative findings [1,2]. Currently, the literature is minimal when it comes to emphysematous osteomyelitis of the foot, with the first article being identified in 2014 [5]. Subcutaneous emphysema is typically described concurrently with patients presenting with emphysematous osteomyelitis, with a report of both present at 79% [6]. Compared to typical osteomyelitis, when cortical destruction and periosteal reaction may be suggestive signs, emphysematous osteomyelitis may be present without cortical destruction [6]. Computed tomography is currently considered the gold standard for proper identification, similar to cases of necrotizing soft tissue infections [1,2,5]. Currently, the most common identifying feature to help with proper identification of infectious intramedullary air is the “Pumice Stone” sign identified by Small et al. in 2018. It is described as irregularly irregular-sized 2-5mm gas locules and was accurately shown in 96% of cases with emphysematous osteomyelitis [6].


Monomicrobial emphysematous osteomyelitis is most associated with hematogenous spread, with anaerobes or Enterobacteriaceae species being the primary contributor [3]. Polymicrobial is associated with contiguous spread, with the most common species being identified as anaerobes or a member of the Enterobacteriaceae species [3]. The patient presented in our case aligns with the current conventional thought, as this patient likely developed his infection secondary to contiguous spread, with polymicrobial growth on culture. However, our patient did not grow anaerobes and some gram-negative organisms were not worked up to identify as Enterobacteriaceae, which the literature currently suggests being most identified [3].
Our case study provides a unique presentation of emphysematous osteomyelitis of the foot. To the author’s knowledge based on a thorough database search, one other article was identified with emphysematous osteomyelitis within the calcaneus, which concurrently presented with subcutaneous emphysema [7]. The patient in the Gruenberg case study, unfortunately, required above-knee amputation after serial debridement’s secondary to the extent of the infection [7]. Our patient had a dissimilar presentation of their calcaneal infection, as there was no surrounding subcutaneous emphysema (Figure 2) but did require a below-knee amputation. The difficulty with our patient was that the infection was not easily identifiable on plain radiographs, leading to a delay in diagnosis until advanced imaging was completed. There is no agreement in the current literature on the use of plain radiographs for accurate identification of emphysematous osteomyelitis. Once the diagnosis of emphysematous osteomyelitis was made, a multi-disciplinary team was assembled that included podiatry, vascular surgery, infectious diseases, and medicine team, allowing prompt, decisive decision-making and urgent intervention that saved the patient from a more proximal amputation or worse fate.
Unfortunately, without clinical evidence of necrotizing soft tissue infection or subcutaneous emphysema noted on plain radiographs, there remains difficulty of when computed tomography should be indicated for assessment of intraosseous air. Future research regarding what laboratory studies and clinical features may need to be identified to help assess for emphysematous osteomyelitis when there is no concurrent subcutaneous emphysema.
Conclusion
Emphysematous osteomyelitis remains a significantly rare foot manifestation, but a life-threatening complication in patients with diabetic foot ulcers, with a high risk of proximal amputation and mortality. It remains a diagnostic challenge due to a lack of reliable findings on plain radiographs, limited awareness, and sparse literature. Our case provides knowledge towards an atypical presentation without subcutaneous emphysema, highlighting the need for further diagnostic assistance when advanced imaging may not be immediately accessible. Still, the current treatment is urgent surgical resection and antibiotics initiation, which makes limb salvage extremely difficult. Further identification of laboratory studies and clinical features may assist in earlier detection when intraosseous air is not identified on plain radiographs.
Conflict of interest: There are no conflicts of interest.
References
- Raju R, Kani K, Lischuk A, Wang A, Porrino J. Imaging of emphysematous osteomyelitis. PMR. 2019; 11: 322-324.
- Garrido Márquez I, Moyano Portillo Á, Acosta Martínez Del Valle MA, Rodríguez Madroñal G, Pérez Cuenca E. Emphysematous osteomyelitis: a rare and aggressive disease. Radiologia (Engl Ed). 2023; 65: S71-S73.
- Luey C, Tooley D, Briggs S. Emphysematous osteomyelitis: a case report and review of the literature. Int J Infect Dis. 2012; 16: e216-e220.
- Giurato L, Meloni M, Izzo V, Uccioli L. Osteomyelitis in diabetic foot: a comprehensive overview. World J Diabetes. 2017; 8: 135142.
- Bhattarai V, Acharya K, Kuikel S, Mahat S, Agarwal S, Ghimire R, Poudel ASK. Radiologic finding of intraosseous gas: a rare case of emphysematous osteomyelitis of the foot. Radiol Case Rep. 2022; 18: 643-646.
- Small JE, Chea P, Shah N, Small KM. Diagnostic features of emphysematous osteomyelitis. Curr Probl Diagn Radiol. 2022; 51: 666-672.
- Gruenberg KM, Halgas BJ, Lundy J. Emphysematous osteomyelitis of the calcaneus: a case report and review. Int J Burns Trauma. 2022; 12: 185-187.