
Open Journal of Clinical and
Medical Images
Case Report - Open Access, Volume 5
Rare type of persistent truncus arteriosus (pulmonary atresia with ventricular septal defect): A case report
Hussain M Alnemer*
Department of Medical Imaging, Dammam Medical complex, Saudi Arabia.
*Corresponding Author: Hussain M Alnemer
Department of Medical Imaging, Dammam Medical complex, Saudi Arabia.
Email: hmalnemer@moh.gov.sa, hussaintiger@gmail.com
Received : Jul 21, 2025
Accepted : Aug 21, 2025
Published : Aug 28, 2025
Archived : www.jclinmedimages.org
Copyright : © Alnemer HM (2025).
Citation: Alnemer HM. Rare type of persistent truncus arteriosus (pulmonary atresia with ventricular septal defect): A case report. Open J Clin Med Images. 2025; 5(2): 1209.
Clinical history
20 years old gentleman known to have a congenital heart disease presenting with a chronic history of hypoxemia. Presenting with dyspnea for 5 days.
Imaging findings
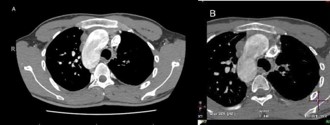
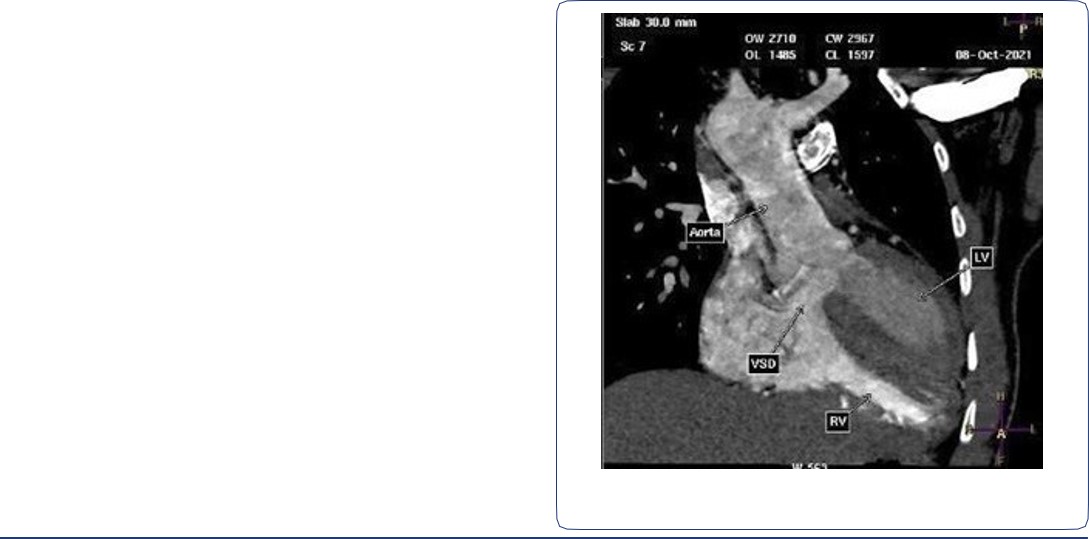
CT angiogram of chest shows complex cardiac disease including right-sided aortic arch (Figure 1), ventricular septal defect and overriding aorta (Figure 2). Non-visualization of the pulmonary trunk (Figure 3).
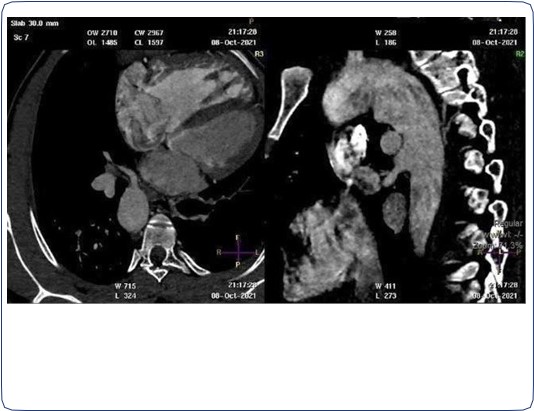
Two arterial supplies to the right lung arising from the descending aorta. A dominant one arising from the medial side that supplies the right upper lobe (Figure 3). Another smaller branch supplies the right middle and lower lobes (Figure 4).
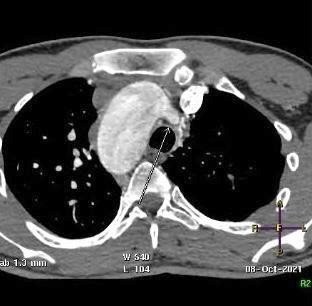
Small blind-ended artery arising from the aortic arch at the take-off point of the left brachiocephalic artery (Figure 5) with non-visualization of left main pulmonary artery (Figure 3A). Multiple small arterial collaterals at the left hilum supplying the relatively hypo-plastic left lung (Figure 3A).
Right ventricular dilatation with myocardial hypertrophy (Figure 4).

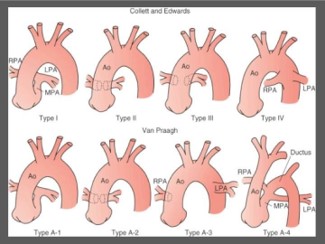
Ao: Ascending Aorta; LPA: Left Pulmonary Artery; MPA: Main Pulmonary Artery; RPA: Right Pulmonary Artery.
(Adapted from St Louis, JD: Persistent truncus arteriosus. In Nichols DG, Ungerleider RM, Spevak PJ, et al [eds]: Critical heart disease in infants and children, Philadelphia, 2006, Mosby, p 690.)
Discussion
Background
Truncus arteriosus is a congenital heart defect characterized by a single arterial trunk arising from the heart, which supplies both the systemic and pulmonary circulation. This anomaly results from the failure of the embryonic truncus arteriosus to divide into the aorta and pulmonary artery during the early stages of fetal development. Pathophysiologically, the presence of a single vessel leads to mixed oxygenated and deoxygenated blood flow, causing systemic hypoxemia and volume overload of the lungs. The condition is often associated with other cardiac anomalies, particularly Ventricular Septal Defects (VSD) and is commonly classified into four types based on the anatomy of the pulmonary artery branches [1,2].
Clinical perspective
Children with truncus arteriosus typically present with symptoms of heart failure, including tachypnea, cyanosis, and poor feeding. The clinical problem arises from the risk of pulmonary over circulation and congestive heart failure if left untreated. Imaging is crucial for diagnosis and preoperative assessment, as it helps delineate the anatomy of the great vessels and associated defects. Clinicians must convey the urgency of obtaining high-quality imaging to assess the hemodynamic status and the need for surgical intervention [3].
Imaging perspective
Key imaging modalities include echocardiography, which is often the first-line tool, followed by cardiac MRI and CT angiography for detailed anatomical assessment. Diagnostic pearls include identifying the morphology of the truncus arteriosus, assessing the VSD size, and evaluating pulmonary blood flow. Final diagnosis is typically confirmed through echocardiographic findings, supplemented by other imaging techniques to provide comprehensive anatomical visualization [4,5].
Types
The Collett and Edwards system [6] is the earliest form of classification, developed in 1949. It is based on where pulmonary arteries arise from the common trunk.
- Type I: The main pulmonary is present and bifurcates into the left and right pulmonary arteries (most common) (same as Van Praagh type A1)
- Type II: The right and left branches arise adjacent to each other from the posterolateral segment of the common trunk (second most common) (same as Van Praagh type A2)
- Type III: The right and left branches originate separately from the right and left lateral segments of the common trunk (as opposed to posterior trunk) (this type is included in Van Praagh type A2).
- Type IV: Neither of the branches arise from the common trunk, but are perfused by aortopulmonary collaterals. This type is now categorized as a form of pulmonary atresia with a ventricular septal defect rather than TA.
Outcome
Therapeutic options primarily involve surgical intervention, usually performed in the first few months of life. The procedure typically entails truncal valve repair or replacement and reconstruction of the pulmonary arteries. Prognosis significantly improves with timely surgical intervention, although lifelong follow-up is necessary due to potential complications like pulmonary hypertension and residual valve dysfunction. Imaging plays a pivotal role in preoperative planning and postoperative monitoring, ensuring optimal outcomes [7,8].
Take home message/Teaching points
Truncus arteriosus is a critical congenital heart defect requiring prompt diagnosis and intervention. Understanding the anatomy through imaging is essential for effective treatment planning. Clinicians should remain vigilant for signs of heart failure in infants and prioritize echocardiography to facilitate early detection and management. Ongoing follow-up with advanced imaging modalities is essential for long-term care [9].
Final diagnosis: Complex cardiac disease with type IV trucus arteriosus (Pulmonary atresia with ventricular septal defect). (Figure 6)
Differential diagnosis: Tetralogy of Fallot with Pulmonary artery atresia.
References
- M A S, et al. Congenital heart defects: epidemiology and clinical management. Pediatr Cardiol. 2022.
- R S, et al. Truncus arteriosus: clinical and pathophysiological considerations. J Cardiovasc Med (Hagerstown). 2023.
- J T, et al. Imaging in congenital heart disease: a practical guide. Radiol Clin North Am. 2021.
- A B, et al. Echocardiography in congenital heart disease. Heart. 2022.
- K C, et al. Role of MRI in congenital heart disease. Eur Heart J. 2020.
- Collett RW, Edwards JE. Persistent truncus arteriosus; a classification according to anatomic types. Surg Clin North Am. 1949;29:1245-1270.
- L D, et al. Surgical management of truncus arteriosus. Ann Thorac Surg. 2023.
- F E, et al. Long-term outcomes in patients with truncus arteriosus. J Thorac Cardiovasc Surg. 2021.
- P Q, et al. Follow-up strategies in congenital heart disease. Pediatr Health Med Ther. 2020.