
Open Journal of
Clinical and Medical Images
Case Report - Open Access, Volume 3
Megalencephalic leucoencephalopathy with subcortical cysts: A cause of early seizures after trivial head trauma
Elena Pasini*; Patrizia Riguzzi; Roberto Michelucci
Unit of Neurology, IRCCS Istituto delle Scienze Neurologiche di Bologna, Italy.
*Corresponding Author: Elena Pasini
Unit of Neurology, IRCCS Istituto delle Scienze Neurologiche Via Altura, 3 Bologna, Italy.
Tel: 0039-051-6225368;
Email: elena.pasini@isnb.it
Received : Aug 24, 2023
Accepted : Sep 12, 2023
Published : Sep 19, 2023
Archived : www.jclinmedimages.org
Copyright : © Pasini E (2023).
Abstract
Megalencephalic Leucoencephalopathy with subcortical Cysts (MLC) is a rare autosomal recessive disease with onset in infancy. Typically, the first symptom is macrocephaly which becomes evident in the first year of life [1-3]. After several years, usually within the first decade of life, slowly progressive ataxia, pyramidal signs, mild cognitive impairment and sporadic seizures complete the phenotype. Diagnosis is suggested by the peculiar aspect of brain MRI showing extensive alterations in white matter along with subcortical cysts in temporo-parietal regions [1,3,4] and is confirmed by genetic tests on MLC1 gene [5,6].
The overall prognosis of this condition is dismal, with most patients becoming wheel-chair dependent as teenagers. Due to this invalidating course, most studies of MLC are confined to infancy/ childhood but adult cases, although rarely, have been reported [7- 12].
At variance with other leucoencephalopathies, epileptic seizures are common in MLC, accounting for about 60% of the patients, but systematic studies of long-term follow-up are lacking [13].
Here we describe two adult sisters with MLC, aged respectively 46 and 43 years, showing recurrent seizures evoked by cranial trauma.
Citation: Pasini E, Riguzzi P, Michelucci R. Megalencephalic leucoencephalopathy with subcortical cysts: A cause of early seizures after trivial head trauma. Open J Clin Med Images. 2023; 3(2): 1138.
Case reports
The first-born sister showed macrocephaly since her birth. At the age of 4 years, she had her first tonic clonic seizure after a minor head injury; at the age of 6 years, she had a convulsive status epilepticus preceded by an accidental fall with minor head trauma. Since then she underwent a rapidly progressive psychomotor regression which forced her to wheel-chair at the age of 7. When she was 14, another minor head injury was immediately followed by tonic-clonic seizures and subsequently by progressive pseudobulbar syndrome and tetraplegia. Since the age of 25 years the patient was bedridden. When admitted in our Neurology Unit at the age of 46, neurological examination showed severe cognitive impairment, mutism, spastic laughing and crying, slow saccades, horizontal nystagmus and spastic tetraplegia. She died at the age of 47 years due to bronchopneumonia.
The younger sister manifested macrocephaly since the age of four months and ataxic gait since the age of 2 years. One year later, a minor head trauma was followed by a tonic-clonic seizure. Progressive psychomotor impairment developed over the years causing inability to walk and wheel-chair use since the age of 7 years. A more severe cognitive and neurological decline with emotional lability, mutism, dysphagia and tetraplegia occurred in her fourties. When admitted at our Neurology Unit at the age of 43, neurological examination was strictly similar to that of her sister, showing marked cognitive impairment, inability to speak and understand verbal messages, horizontal nystagmus, spastic crying and laughing, tetraplegia.
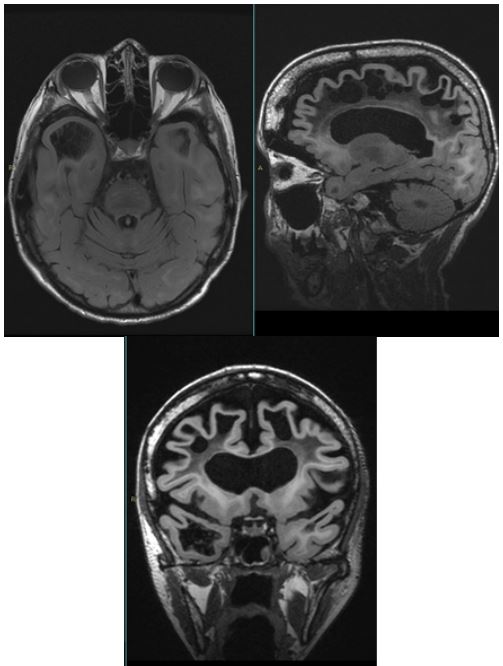
Both patients were on chronic treatment with valproate. No abnormalities were found in interictal awake and sleep EEGs aside from diffuse slowing. Cerebral MRI respectively at 46 and 43 years old, showed extensive alterations in white matter and subcortical cysts in fronto-temporo-parietal regions (Figures 1 and 2).
MLC1 gene mutation screening confirmed an homozygous mutation (c.423+1g>a) in both sisters.

Cerebral MRI images of the older sister show severe leukoencephalopathy with supratentorial white matter spongiform degeneration. Multiple cystic formations are visible in the frontal, parietal and temporo-polar areas. The U-shaped fibers are involved, and a thin brain cortical mantle remains with swelling of the convolutions. Moderate cerebellar atrophy, marked dilatation of the lateral ventricles, enlargement of subarachnoid spaces of the convexity and cisterns are also observed.
Cerebral MRI images of the younger sister show a severe, albeit less prominent than the sister, leukoencephalopathy with multiple cystic formations and dilatation of the lateral ventricles. The subarachnoid spaces of the convexity and cisternal spaces are enlarged.
Discussion
In this paper we describe two adult sisters suffering from MLC and showing the typical phenotype of macrocephaly in the first months of life followed by progressive neurological dysfunction leading to severe psychomotor handicap (with wheelchair dependency since the age of 7 years).
Both sisters had sporadic epileptic seizures, invariably precipitated by minor head trauma. The seizures were apparently generalized tonic-clonic seizures and occurred usually as isolated, sporadic events or in the form of convulsive status epilepticus in one occasion. Interestingly the seizures (especially the status) heralded an acute or progressive sustained neurological deterioration and seemed to be associated with a more rapid worsening of the condition. A the time of our observation the routine and sleep EEGs were unrevealing.
The analysis of the MLC cases reported in the literature shows that “epilepsy” is a common feature of MLC, occurring in about 60% of cases [13]. The age of onset of epilepsy ranges between 1,5 and 14 years and seizures are mostly generalized tonic-clonic (sometimes with a clear focal onset). Myoclonic, atonic and complex partial seizures have been reported in a few patients [5,14-16]. The seizures are usually sporadic and easily controlled with antiepileptic therapy but cases with refractory seizures and status epileptics have been described. Interestingly trauma has been recognized as a trigger in 10-50% of the previously reported cases. Most patients show EEG abnormalities, usually in the form of spike or polyspike foci in the parietal, temporal and frontal areas with migratory changes in wakefulness and sleep [13]. Abnormal photo-paroxysmal responses are present in some patients.
Among leucodystrophies and other leucoencepahalopathies, the high incidence of epilepsy seems to be a particular feature of MLC [17] and the reason may be related to new insights into the pathogenesis of this condition. Around 75% of patients with MLC are associated with mutations of the gene encoding MLC1, a membrane protein mainly expressed in astrocytes of the CNS regulating the ion flux and fluid and ion homeostasis [18,19]. The astrocyte dysfunction in turns has been quoted to play a role in epileptogenesis through disrupted astrocyte-neurons relationships, uptake and redistribution of ions and water, and glucose metabolism [20]. Therefore it is possible that astrocyte dysfunction may explain this relatively high incidence of epilepsy in this condition [21].
In addition in our patients seizures were precipitated by minor head trauma. In MLC minor head trauma can induce temporary deterioration, most often with seizure or status epilepticus, prolonged unconsciousness lasting days to months or acute motor deterioration [22-24].
Interestingly a syndrome of early seizures after trivial head trauma has been described in infants, usually in combination with sometimes very severe cerebral oedema (“early seizures and cerebral oedema after trivial head trauma” -ESCEATHT) [25]. ESCEATHT has been observed in association with CACNA1 S218L mutation, which may also cause, sometimes in the same patients, hemiplegic migraine attacks and comatose episodes after minor head injury [26]. This mutation causes rather dramatic changes in Cav 2.1 Ca2+ channel function by increasing the cellular influx of Ca2+ and leading to enhanced release of neurotransmitters such as glutamate. As a result of this mutation, even weak and otherwise harmless stimuli (such as minor trauma) may readily depolarize Cav 2.1 Ca2+ channels and trigger severe and protracted cytotoxic cerebral oedema and cell loss [27].
Chronic white matter oedema is the essential feature of MLC, caused by a genetic defect in brain ion and water homeostasis and volume regulation by astrocytes. It may be hypothesized that, in this pathological context of astrocyte dysfunction and impaired water homeostasis, even a minor trauma, by impairing the Brain Blood Barrier function, can easily trigger the cascade of events, involving astrocyte signaling, leading to a seizure.
We suggest that early post-traumatic seizures after trivial trauma are a distinctive clinical condition, suggesting the existence of a genetic cause. In detail this entity cannot be regarded as “epilepsy” (defined as recurrence of unprovoked seizures) but rather characterized by situation-related (provoked) seizures, most frequently caused by MLC1 mutations.
References
- Van der Knaap MS, Parth PG, Stroink H, et al. Leucoencepahalopathy with swelling and a discrepantly mild clinical course in eight children. Ann Neurol. 1995; 37: 324-334.
- Singhal BS, Gursahani RD, Udani VP, Biniwale AA. Megalencephalic leukodystrophy in an Asian Indian ethnic group. Pediatr Neurol. 1996; 14: 291-296.
- Van der Knaap MS, Boor I, Estévez R. Megalencephalic leukoencephalopathy with subcortical cysts: Chronic white matter oedema due to a defect in brain ion and water homoeostasis. Lancet Neurol. 2012; 11: 973-85.
- Gelal F, Call C, Apaydin M, Erdem G. Van der Knaap’s leukoencephalopathy: Report of five new cases with emphasis on diffusion-weighted MRI findings. Neuroradiology. 2002; 4: 625-630.
- Topcu M, Gartioux C, Ribierre F, et al. Vacuolating megaloencephalic leucoencephalopathy with subcortical cysts, mapped to chromosome 22qtel. Am J Hum Genet. 2000; 66: 733-739.
- Leegwater PAJ, Boor PKI, Yuan BQ, et al. Identification of novel mutations in MLC1 responsible for megalencephalic leukoencepahalopathy with subcortical cysts. Hum Genet. 2002; 110: 279-283.
- Itoh N, Maeda M, Naito Y, Narita Y, Kuzuhara S. An adult case of megalencephalic leukoencephalopathy with subcortical cysts with S93L mutation in MLC1 gene: a case report and diffusion MRI. Eur Neurol. 2006; 56: 243-5.
- Saijo H, Nakayama H, Ezoe T, et al. A case of megalencephalic leukoencephalopathy with subcortical cysts (van der Knaap disease): molecular genetic study. Brain Dev. 2003; 25: 362-366.
- Singhal BS. Leukodystrophies: Indian scenario. Indian J Pediatr. 2005; 72: 315-318.
- Singhal BS, Gorospe JR, Naidu S. Megalencephalic leukoencephalopathy with subcortical cysts. J Child Neurol. 2003; 18: 646- 652.
- Pascual-Castroviejo I, van der Knaap MS, Pronk JC, Garcia-Segura JM, Gutierrez-Molina M, et al. Vacuolating megalencephalic leukoencephalopathy: 24 year follow-up of two siblings. Neurologia. 2005; 20: 33-40.
- Joseph E, Sureka J, Gibikote S, Aaron S, Thomas MM. Megalencephalic leucoencephalopathy with subcortical cysts in an adult. Acta Neurol. Belg. 2009; 109: 53-54.
- Yalçinkaya C, Yüksel A, Comu S, Kiliç G, Cokar O, et al. Epilepsy in vacuolating megalencephalic leukoencephalopathy with subcortical cysts. Seizure. 2003; 12: 388-96.
- De Stefano N, Balestri P, Dotti MT, et al. Severe metabolic abnormalities in the white matter of patients with vacuolating megalencephalic leukoencephalopathy with subcortical cysts. A proton MR spectroscopic imaging study. J Neurol. 2001; 248: 403-409.
- Harbond MG, Harden A, Harding B, Brett EM, Baraitser M. Megalencephaly with dysmyelinatiomn, spasticity, ataxia, seizures and distinctive neurophysiological findings in two siblings. Neurpediatrics. 1990; 21: 164-168.
- Higuchi Y, Hattori H, Tsuji M, Asato R, Nakahata T. partial seizures in leukoencephalopathy with swelling and a discrepantly mild clinical course. Brain & Development. 2000; 22: 387-389.
- Goutieres F, Boulloche J, Bourgeois M, Aicardi J. Leukoencephalopathy, megalencephaly and mild clinical course. A recently individualized familial leukodystrophy: report of five new cases. J Child Neurol. 1996; 11: 439-444.
- Patrono C, Di Giacinto G, Eymard-Pierre E, Santorelli FM, Rodriguez D, et al. Genetic heterogeneity of megalencephalic leukoencephalopathy and subcortical cysts. Neurology. 2003; 61: 534-7.
- Lanciotti A, Brignone MS, Bertini E, Petrucci TC, Aloisi F, et al. Atrocytes: Emerging stars in leukodystrophy pathogenesis. Transl Neurosci. 2013; 4.
- Steinhauser C, Seifert G. Astrocyte dysfunction in epilepsy. In: Noebels JL, avoli M, Rogawski MA, Olsen RW, Delgado-Escueta AV (eds) Jasper’s basic mechanisms of the epilepsies, fourth ed. NCBI Bookshelf Online Book Version. 2012; 1-9.
- Brignone MS, Lanciotti A, Visentin S, et al. Megalencephalic leukoencephalopathy with subcortical cysts protein-1 modulates endosomal pH and protein trafficking in astrocytes: Relevance to MLC disease pathogenesis. Neurobiology of Disease. 2014; 66: 1-18.
- Ben-Zeev B, Gross V, Kushir T, et al. Vacuolating megalencephalic leukoencephalopathy in 12 Israeli patients. J Child Neurol. 2001; 16: 93-99.
- Riel-Romero RM, Smith CD, Pettigrew AL. Megalecephalic lekoencephalopathy with subcortical cysts in two siblings owing to two novel mutations: case reports and review of the literature. J Child Neurolo. 2005: 20: 230-234.
- Bugiani M, Moroni I, Bizzi A, et al. Consciousnes disturbances in megalencephalic leukoencephalopathy with subcortical cysts. Neuropediatrics. 2003: 34-211-214.
- Snoek JW, Minderhout JM, Wilmink JT. Delayed deterioration following mild head injury in children. Brain. 1984; 107: 15-36.
- Kors EE, Terwindt GM, Vermeulen FL, et al. Delayed cerebral edema and fatal coma after minor head trauma: Role of the CACNA1A calcium channel subunit gene and relationship with familial hemiplegic migraine. Ann Neurol. 2001; 49: 753-760.
- Stam AH, Luijckx GJ, Poll-Thé BT, et al. Early seizures and cerebral oedema after trivial head trauma associated with the CACNA1A S218L mutation. J Neurol Neurosurg Psychiatry. 2009; 80: 1125-9.