
Open Journal of Clinical and
Medical Images
Case Report - Open Access, Volume 3
Recognizing acquired hemophilia A as a cause of subdural hemorrhage and use of thromboelastography to guide management in neurocritical care unit
Paul B Lee; Taha Ataya; Yuvraj Bhagat; Wazim Mohamed; Syeda Maria Muzammil*
Department of Neurology, Division of Neurotrauma/Neurocritical Care – Detroit Medical Center/Wayne State University, Detroit, MI, USA.
*Corresponding Author: Syeda Maria Muzammil
Department of Neurology, Detroit Medical Center/Wayne State University, USA.
Tel: 313-577-1242;
Email: mmuzammi@med.wayne.edu
Received : Apr 27, 2023
Accepted : Jun 09, 2023
Published : Jun 16, 2023
Archived : www.jclinmedimages.org
Copyright : © Muzammil SM (2023).
Abstract
Acquired Hemophilia A (AHA) is caused by development of autoantibodies against factor VIII. It is a rare disorder with a prevalence of 1.5 per million-year and is important to identify as a potential etiology of intracranial hemorrhage. These patients may just present with an isolated prolongation of activated partial thromboplastin time (aPTT) and no prior history of hemorrhagic disorders. Our case involves a 68-year-old woman transferred to our neurocritical care unit for management of a posterior fossa subdural hemorrhage with re-accumulation post suboccipital craniectomy and evacuation. Noted on initial labs was an isolated prolongation of aPTT that was later confirmed to be factor VIII deficiency secondary to acquired factor VIII inhibitor. We utilized thromboelastography (TEG) to start tailored time-sensitive hemostatic treatment with activated Prothrombin Complex Concentrate (aPCC) or factor VIII inhibitor bypassing activity (FEIBA) and advocate its usage to detect and monitor hypocoagulability.
Citation: Lee PB, Ataya T, Bhagat Y, Mohamed W, Muzammil SM. Recognizing acquired hemophilia A as a cause of subdural hemorrhage and use of thromboelastography to guide management in neurocritical care unit. Open J Clin Med Images. 2023; 3(1): 1112.
Introduction
Hemophilia A is a bleeding disorder characterized by the deficiency of factor VIII in the intrinsic coagulation pathway. The classical form of Hemophilia A is a genetic X-linked disease and predominantly affects males. AHA, however, is a rare condition affecting adults of both sexes due to production of autoantibodies against factor VIII. Acquired factor VIII inhibitors are associated with approximately 1.5 cases per million each year with a large distribution of patients aged 68-80 years [1]. Approximately 50% of AHA cases are idiopathic with all other cases associated with autoimmune diseases such as systemic lupus erythematosus, hematologic malignancy, use of certain medications including penicillin and sulfa antibiotics, and acute hepatitis B and C infections [2]. Intracranial hemorrhage in association with AHA is an even rarer occurrence (1-1.4% of AHA patients) [3]. Therefore, greater awareness and preparation is needed to manage acute intracranial bleed due to acquired factor VIII inhibitors.
Case report
A 68-year-old woman with a history of beta-thalassemia minor presented to her local hospital with severe occipital headaches, and nausea and vomiting. On presentation, she was lethargic but the remainder of her neurological exam was non-focal. She reported bumping her head against furniture about 2 weeks prior, without associated loss of consciousness or subsequent headaches. She additionally noted easy bruisability of her arms and legs since then. She reported no prior history of bleeding disorder, or antiplatelet and anticoagulant use. Initial Computed Tomography (CT) head showed a subdural hemorrhage in the posterior fossa. She subsequently developed declining mentation and underwent an urgent left suboccipital craniectomy for evacuation of hematoma. Immediately post procedure, she was awake and following commands with neurological exam non-focal. This soon progressed to obtundation over the next 2-3 hours. Repeat CT Head showed reaccumulating bleed in the posterior fossa with right intraventricular bleed. A right External Ventricular Drain (EVD) was inserted and the patient was taken back to the operating room for extension of craniectomy and C1 laminectomy with no improvement in neurological status. Patient was subsequently medi-flighted to our hospital’s neurocritical care unit.
On arrival, the exam was noted for absent brainstem reflexes with significant bruising over arms and legs. Osmotic therapy was immediately initiated with mannitol and 23.4% hypertonic saline. CT Head showed bilateral posterior fossa subdural hemorrhage greater on the left measuring maximum 9 mm with right intraventricular hemorrhage and right EVD in place (Figure 1). There was also diffuse cerebral edema with 6 mm midline shift to the left. Admission labs showed a normal Prothrombin Time (PT) and International Normalization Ratio (INR), but aPTT was significantly prolonged at 53.2 seconds. Hematology was contacted for suspicion of acquired factor deficiency. In the interim, TEG study was ordered (Figure 6) and showed prolonged R time, K time and decreased alpha angle and maximum amplitude, suggestive of factor deficiency with impaired fibrin cross-linking, overall decreased clot formation and platelet function. 50 units/kg of aPCC/FEIBA was given. Mixing studies were ordered and showed a continued prolongation of aPTT representing a time-dependent inhibitor in the intrinsic pathway. Factor IX activity was normal but factor VIII activity was undetectable with high titer of factor VIII inhibitor at 12.9 Bethesda Units/mL (BU/mL). 50 units/kg of factor VIII was given to increase factor VIII levels and aPCC/FEIBA 50 units/kg every 6 hours was given for hemostasis. Additional treatment included continuous infusion with norepinephrine for blood pressure support and vasopressin for central diabetes insipidus.
24-hour repeat CT Head (Figure 2) showed mildly decreased hydrocephalus with stable bilateral residual subdural hematoma in posterior fossa with 6 mm midline shift to the left. However, hypodensity was evident in bilateral cerebellum and brainstem greater on the left, likely due to ischemia. Physical exam showed 6 mm fixed dilated pupils with only a few spontaneous breaths and triple flexion in bilateral lower extremities. Meeting was held with the patient’s family and a decision was made for withdrawal of care and compassionate discontinuation of life-sustaining mechanical ventilation. Patient expired soon afterwards. Laboratory testing on blood samples obtained prior to death was strongly positive for Antinuclear Antibody (ANA).
Discussion
AHA leading to intracranial hemorrhage is a hematological and neurological emergency. Prompt recognition of AHA as a cause is important so that timely treatment can be instituted prior to neurological surgery and in the post-operative period. Table 1 summarizes the to-date six cases that have been reported in literature describing experience with diagnosing and managing AHA related subdural hemorrhage with patients not on anticoagulation. Higher mortality is noted in instances where neurosurgical procedures are required emergently.
Isolated prolonged aPTT in older individuals with intracranial hemorrhage could point to an acquired deficiency of clotting factors or presence of factor inhibitors (Figure 3). Hematology should be consulted with mixing studies ordered to differentiate between acquired factor deficiency and presence of an inhibitor (Figure 4). When aPTT does not correct with mixing studies, this points towards the presence of an inhibitor, and factor inhibitor autoantibodies plus factor VIII level should be measured to confirm the diagnosis. Emergency medicine physicians, who are often the first point of contact of these patients, should be particularly alert to diagnosing and managing acquired hemophilia. Quite often these patients may end up going for emergent neurosurgical procedures soon after their first encounter in the emergency department. This makes it critical to recognize this disease and achieve hemostasis with bypassing agents prior to any invasive procedures. In the case of our patient, earlier diagnosis would have been made if a coagulation screen had been performed at initial presentation, especially in the context of abnormal bruising, which would have allowed hemostatic treatment to prevent bleeding at the time of the first operation and prevent post-operative re-bleeding.
We incorporated the use of TEG to measure the in-vivo clotting function of the whole blood as a supplement to conventional aPTT to guide transfusion of blood products. Figure 5 shows a representative waveform of a normal TEG tracing. R time is the latency until clot formation begins with 2 mm amplitude, K time is the time from R until the clot reaches 20 mm, alpha angle shows the rate at which fibrin cross linking occurs, MA (maximum amplitude) shows the highest point on the TEG curve indicating maximum clot strength, and LY30 shows fibrinolytic activity 30 minutes after MA [9,10]. aPCC was subsequently administered which, of note, has been recommended to use as a bypassing agent in AHA patients [9]. In a time-sensitive scenario, TEG may guide tailored management as mixing studies take 3-4 hours to conclude and result. In addition, since the coagulation parameters such as aPTT normalizes when levels of factor VIII are over 30-50%, the severity of bleeding cannot be predicted based on factor VIII activity or inhibitor levels alone [10]. Although our patient passed away soon after, TEG would have served as an important tool to monitor hemostasis and limit the amount of blood products administered.
The next step for treatment regarding acquired hemophilia would be to eradicate the inhibitor usually either with prednisone with or without cyclophosphamide [1]. In addition, the underlying cause of the disease, if there is any, should be addressed [2]. In our patient’s case, ANA antinuclear antibody was strongly positive just before her death which may suggest an autoimmune disorder contributing to the formation of factor VIII inhibitor. Although 50% of all cases are labeled as idiopathic, further autoimmune workup would have been warranted for this patient after stabilization to address the underlying source of AHA. A pathway for evaluation and management is suggested (Figure 7).






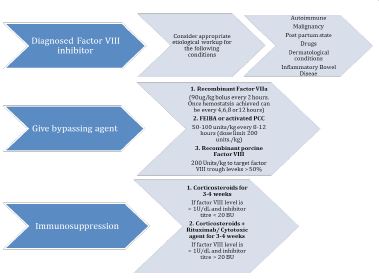
Table 1: The course of endoscopic treatments.
| Author (year) | Past medical history | Patient presentation | Location of hemorrhage | Hematologic labs | Treatment and outcome |
|---|---|---|---|---|---|
| Kitamura (2018) [3] | 93-year-old woman with no prior bleeding history | Headache after likely suffering fall, had persistent hemorrhage at tooth extraction site 8 days prior | Acute subdural hematoma on right frontal lobe | aPTT: 70.7 sec Factor VIII activity: 9% Factor VIII inhibitor: 7 Bethesda Units/mL Repeat aPTT and FVIII activity levels: 52.9 sec and 35% respectively | Did not start prednisone. Fresh Frozen Plasma (FFP) infused. aPTT and FVIII activity levels were significantly improved. Hematoma gradually increased. Patient had decreased levels of consciousness and died 13 days after admission |
| Yek (2017) [4] | 44-year-old man with a history of Idiopathic Thrombocytopenia Purpura (ITP) and Thrombotic Thrombocytopenic Purpura (TTP) | Sudden onset headache, left pupil was 5 mm in diameter while the right was 3 mm | Acute right subdural hemorrhage with midline shift | aPTT: 125.4 seconds Factor VIII activity: undetectable Factor VIII inhibitor: > 700 Bethesda units/mL | Patient was started on aPCC/FEIBA every 12 hrs for 4 days. Platelet transfusion given daily for 10 days. Also given immunosuppressive therapy with rituximab 375 mg/m^2 weekly for 4 weeks, cyclophosphamide 50 mg daily, hydrocortisone 100mg every 8 hours and Intravenous Immunoglobulins 50 gm per day for two days. Patient achieved full neurological recovery on conservative management. |
| Sehara (2015) [5] | 80-year-old man no bleeding history | Left hemiplegia, fall, and seizures | Right hemispheric subdural hematoma | aPTT: 104.2 sec Factor VIII activity: 4% FVIII inhibitor: 3 Bethesda Units/mL | Initially Fresh Frozen plasma and red blood cell concentration were transfused. After repeat studies determined the patient to be positive for AHA, the patient was treated with methylprednisolone pulse therapy with 1 g per day for 3 days, followed by oral prednisolone therapy (1 mg/kg body weight). Patient had improvement in clinical picture with correction of FVIII activity and undetectable FVIII inhibitor on repeat testing. |
| Kim (2010) [6] | 49-year-old man with history of HTN and Diabetes | Originally presented with upper and lower extremity hemorrhage in the context of consuming 10 g of dried gallbladder of a cobra. One year later presented with upper extremity swelling and sudden loss of consciousness. | Subdural hematoma in the left fronto-temporo-occipital areas | aPTT: 120 sec Factor VIII activity: less than 1% Factor VIII inhibitor: 217 Bethesda Units/mL | Recombinant factor VII was infused. Despite treatment, the patient’s bleeding worsened. Two weeks later, developed multifocal subarachnoid hemorrhages and bilateral intracranial hemorrhages. He subsequently died. |
| Micic (2010) [7] | 86-year-old woman with no bleeding history | Severe occipital headache, dysarthric speech, nausea, and hypertensive with systolic blood pressure > 200 mm Hg | Right cerebellar intraparenchymal hemorrhage without midline shift Repeat CT showed a posterior fossa bleed with extension into the contralateral left cerebellum, and a secondary right frontal hemorrhage at the site of frontal ventriculostomy | aPTT: 53.4 sec Postmortem testing showed Factor VIII activity 13% and positive Factor VIII inhibitor at 1.7 Bethesda Units/mL | Patient underwent an occipital decompressive craniectomy with evacuation of the right cerebellar intraparenchymal hemorrhage and placement of a right frontal ventriculostomy. 8 hours following surgery, her status suddenly declined with loss of all cranial nerve function and an acute drop in blood pressure to 70 mmHg systolic. An emergent CT scan demonstrated a very large posterior fossa bleed with extension into the contralateral left cerebellum, and a secondary right frontal hemorrhage at the site of the frontal ventriculostomy. The patient expired soon afterward. |
| Mashiko (2009) [8] | 74-year-old man no bleeding history | Found comatose in his bed. | Subdural hematoma in the left frontotemporal lobe with significant midline shift Subsequent subdural hematoma in the left posterior temporal lobe Later thalamic hemorrhage | APTT: 77 sec Factor VIII activity: 1% Factor VIII inhibitor: 46 Bethesda Units/mL | Subdural hematoma was surgically evacuated. Following surgery, subcutaneous and epidural hematomas developed a few hours later. Due to repeated hematomas, factor VIII and factor IX concentrates were given. Thalamic hemorrhage occurred on the 9th hospital day. The patient died on the 16th hospital day. |
Conclusion
From review of literature and our case, AHA related intracranial hemorrhages are devastating with mortality particularly higher in surgically managed cases. It is important for patients who present with unexplained intracranial hemorrhage with elevated aPTT to be transferred preferably to a neurocritical care unit. We advocate using TEG to characterize hypocoagulability and consulting hematology for effective management prior to surgical treatment. Neurosurgical procedures are high risk in these patients and frequently complicated by re-bleed.
Key points
1. Acquired Hemophilia A (AHA) is a rare disorder and is important to identify as a potential etiology of intracranial hemorrhage.
2. Prompt diagnosis, and management of AHA with hemostasis, is crucial to establish prior to any invasive procedures.
3. We advocate for the use of Thromboelastograophy (TEG) to monitor hypocoagulability in setting of elevated activated partial thromboplastin time (aPTT).
4. Higher mortality is noted in AHA patients who are managed surgically.
References
- Giangrande P. Acquired hemophilia: Revised Edition. World Federation of Hemophilia. 2012.
- Constantinescu C, Jitaru C, Pasca S, Dima D, Dirzu N, et al. Unexplained hemorrhagic syndrome? consider acquired hemophilia A or B. Blood Reviews. 2022; 53: 100907.
- Kitamura T, Sato T, Ikami E, Fukushima Y, Yoda T. A case of a patient who is diagnosed with mild acquired hemophilia a after tooth extraction died of acute subdural hematoma due to head injury. Case Reports in Dentistry. 2018; 1-3.
- Yek JL, Grant D, He YK, Ng HJ, Tan TK. A difficult case of acquired haemophilia with concomitant Evan’s syndrome presenting with acute subdural haematoma. Haemophilia. 2017; 23.
- Sehara Y, Hayashi Y, Mimuro J. Acquired hemophilia a with a rare presentation of acute subdural hematoma. Case Reports in Neurological Medicine. 2015; 1-4.
- Kim HJ, Lee WS, Lee YJ, Jun HS, Seo SK, et al. Acquired factor VIII deficiency after consuming the dried gallbladder of a cobra, naja naja. The Korean Journal of Hematology. 2010; 45: 205.
- Micic D, Williams EC, Medow JE. Cerebellar hemorrhage as a first presentation of acquired hemophilia a. Neurocritical Care. 2015; 15: 170-174.
- Mashiko R, Yamamoto T, Sato M, Noguchi S, Matsumura A. Acquired hemophilia first manifesting as life-threatening intracranial hemorrhage-case report. Neurologia Medico-Chirurgica. 2009; 49: 93-95.
- Mingot-Castellano ME, García-Candel F, Benítez-Hidalgo O, Marco A, Méndez Navarro GA, et al. Activated prothrombin complex concentrate to treat bleeding events in acquired hemophilia A: BAHAS study. Eur J Haematol. 2022; 109: 686-695.
- Fisher C, Mo A, Warrillow S, Smith C, Jones D. Utility of thromboelastography in managing acquired factor VIII inhibitor associated massive haemorrhage. Anaesthesia and Intensive Care. 2013; 41: 799-803.